End-of-Life Care: Use of Antineoplastic Therapy and Nonessential Medications in Veteran Patients Receiving Palliative Care
Background: The use of antineoplastic therapy and nonessential medications at the end of life can lead to poorer quality of life for patients, decreased satisfaction with care among caregivers, financial toxicity, increased use of the emergency department, and hospitalization.
Objectives: This study evaluated the incidence of antineoplastic therapy administration and use of nonessential medications at 30 and 14 days prior to death among patients with metastatic lung, prostate, colon, or pancreatic cancer who were also receiving palliative care.
Methods: Using retrospective chart review, this study evaluated patients admitted to a U.S. Department of Veterans Affairs healthcare system during a two-year period. Variables assessed included use of antineoplastic therapy and nonessential medications, emergency department visits, hospitalizations, palliative care accessibility, and hospice referrals.
Findings: All patients in the study (N = 57) received palliative care. Sixteen percent of patients in this study received antineoplastic therapy, 14% received nonessential medications, and 40% were hospitalized or visited the emergency department within 30 days of death.
Jump to a section
The use of antineoplastic therapy and nonessential medications are common at the end of life. Studies have not confirmed improved quality of life or a meaningful extended survival. Rather, antineoplastic therapy use near the end of life has been associated with more aggressive care with no improved outcomes and unnecessary healthcare expenditures.
A study by Mack et al. (2015) using the New York State Cancer Registry and Medicaid data among patients diagnosed with stage I–IV cancer revealed that 38% of patients received chemotherapy within 14 days of death, 75% of patients received aggressive care within 30 days of death (defined as an intensive care unit [ICU] admission, hospitalization, or emergency department visit), and only 23% received hospice care before death. Mack et al. (2015) further reported that aggressive end-of-life measures have been associated with poorer quality of life and less caregiver satisfaction with care.
A review by Green et al. (2017) of 21,894 patients diagnosed with stage IIIB or IV non-small cell lung cancer using the Surveillance, Epidemiology, and End Results Program (SEER)–Medicare database reported that 43% received chemotherapy within 30 days of death. Green et al. (2017) went on to conclude that early palliative care intervention can lead to care that is more consistent with the patient’s goals, significantly decreasing chemotherapy use close to death and minimizing the risk for more burdensome side effects.
The findings from this study will help show the benefits of palliative care involvement in improving comprehensive cancer care among patients with stage IV malignancies receiving care from a medical center within the U.S. Department of Veterans Affairs (VA) system. The findings will help promote high-quality end-of-life care and minimize costly and unnecessary aggressive care near the end of life.
Background
A systematic literature review conducted by Clarke et al. (2015) revealed that factors influencing the decision to stop antineoplastic therapy include worsening patient condition and functionality, chemotherapy responsiveness of the tumor, and willingness of the patient and oncologist to acknowledge and discuss that end of life is near. Based on Clarke et al.’s (2015) review, antineoplastic therapy near the end of life is less likely to occur with palliative care.
According to Prigerson et al. (2015), the American Society of Clinical Oncology (ASCO) recommended against the use of chemotherapy in patients with solid tumors who have not benefited from previous treatment and have an Eastern Cooperative Oncology Group (ECOG) performance status score of 3 or more (confined to bed or chair more than 50% of waking hours and capable only of limited self-care). The ASCO recommendations were based on the results of studies conducted in the 1980s that found that chemotherapy use among patients with poor performance status led to low response rates, high rates of toxicities, and shorter survival (Prigerson et al., 2015). Because of these same studies, clinical trials have been targeted toward patients with good performance status, resulting in a lack of information on the benefits and harms of chemotherapy use among patients with poor performance status.
A study by Prigerson et al. (2015) on patients with end-stage cancer who had good performance status and received chemotherapy reported that the patients had a worse quality of life before death as compared to similar patients who did not receive chemotherapy. The study also reported that more than 50% of these patients who went on to receive chemotherapy showed no difference in survival after controlling for clinical setting (receiving intensive care, such as the use of ventilation or resuscitation) and the patient’s performance status.
Bao et al. (2018) found that previous clinical trials in patients with metastatic pancreatic cancer showed a median survival of 8 to 11 months from the time of diagnosis with use of combined chemotherapy versus 6 to 7 months for patients who were treated with a single agent. They also found that chemotherapy use was associated with increased rates of hospital admissions, emergency department visits, death in a hospital, fewer days in hospice care, and a more than 50% increase in out-of-pocket costs for patients. Healthcare costs and use were higher among those who received chemotherapy within the last 30 days of life.
Clarke et al. (2015) found that decisions to discontinue treatment are made over time and fostered by an ongoing and trusting relationship between the patient and their oncologist. An observational cohort study conducted by Margolis et al. (2017) among 5,873 patients who died from uterine cancer using the SEER-Medicare data showed that 7% received chemotherapy within 14 days of death, 55% received aggressive care within 30 days of death, and 66% were referred to hospice prior to death. They also found that there is a large financial burden associated with cancer care in the U.S. healthcare system at the end of life. They added that the transition to end-of-life care starts with a good discussion and that use of palliative care leads to less high-intensity care at the end of life.
A retrospective cohort study by Mor et al. (2016) showed that studies conducted with veteran patients who received palliative or hospice care indicated that they reported better quality of life than those who did not. A study by Ersek et al. (2017) among 847 veteran patients diagnosed with stage IV non-small cell lung cancer reported that 72% received at least one episode of aggressive care and 31% received chemotherapy within the last 30 days of life. They also found that families rated the quality of care lower for those who received aggressive care in the last 30 days of life versus those who did not.
Lindsay et al. (2015) conducted a prospective study among 61 patients with cancer who were receiving inpatient palliative care with an estimated life expectancy of less than six months. Of those, 70% were found to be taking at least one potentially inappropriate medication, including antihypertensives, dyslipidemic agents, and complementary alternative medicine. Lindsay et al. (2015) found that the use of these medications at the end of life can cause medication burden, potential side effects, and unnecessary cost to the patient and healthcare system.
Methods
Sample and Setting
This was a multicenter, retrospective cohort study of patients treated at the John D. Dingell VA Medical Center in Detroit, Michigan, who died from July 1, 2016, to June 30, 2018, and were diagnosed with metastatic lung, colorectal, prostate, or pancreatic cancer or melanoma. Patients who were aged younger than 18 years or older than 90 years were excluded from the study, as were patients who did not receive antineoplastic therapy from the VA and those who received non-VA care.
Procedure
This study was conducted after receiving approval from the John D. Dingell VA Medical Center’s research and development committee and the institutional review board at Wayne State University in Detroit. Because this study was a retrospective review of electronic health records, a waiver for informed consent and protected health information authorization was requested. Using a retrospective database search, 65 patients meeting the general inclusion and exclusion criteria were screened for eligibility, and 57 patients were found to be eligible for the study. De-identified retrospective data were collected via electronic health record review and were stored in a password-protected spreadsheet.
Data were collected by the principal investigator and included the use of palliative antineoplastic therapy and nonessential medications near the end of life (30 days prior to death) among veterans diagnosed with metastatic lung, prostate, colon, or pancreatic cancer or melanoma at 30 and 14 days prior to death who were also receiving palliative care. Information was also gathered on the age and performance status of the patients because these factors have been found to contribute to patient outcomes. The use of aggressive care near the end of life, including hospitalizations and emergency department visits within 30 days of death, and the timeliness of hospice involvement (referral for initiation of hospice services) were also evaluated. Data on the use of antineoplastic therapy (e.g., cytotoxic chemotherapy, oral antineoplastic therapy, immunotherapy) and nonessential medications (e.g., lipid-lowering agents, oral bisphosphonates, vitamin supplements, antiplatelet agents, antidementia medications, gastric protectors without indication, oral antidiabetic agents with most recent hemoglobin A1C of 8% or less, therapeutic duplications) were also obtained. Once all data were collected, the analysis was performed. Data were analyzed using descriptive statistics.
Results
Most of this study’s patients were older adult men. All study patients received palliative care services (see Table 1). Nine patients received chemotherapy within 30 days of death, and three went on to receive chemotherapy within 14 days of death. ECOG scores were available for 46 of the 57 patients, and all available scores were 2. A score of 2 indicates that patients were capable of all self-care but unable to carry out work activities and that they were active for 50% or more of waking hours (Oken et al., 1982).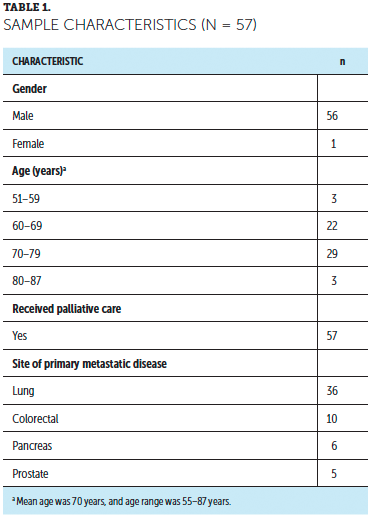
Twenty-five patients had a cancer-related emergency department visit within 30 days of death, and 23 patients were hospitalized 30 days before death. Nine patients died within 6 months of being diagnosed with metastatic disease, 14 died within 6 to 12 months, and 34 died more than 12 months after being diagnosed. Forty-three patients were referred to hospice prior to death. Of the hospice referrals, 10 took place less than 14 days before death, 13 from 15 to 30 days prior to death, and 20 more than 30 days before death. Twenty-two referrals were placed by palliative care, eight by the oncologist, six by the hospitalists, and three by the ICU provider, and four were received from the community where the patients were hospitalized for emergent care. The number of days from hospice referral to death ranged from 1 to 181, with a mean of 40 days.
Eight patients were on nonessential medications within 30 days of death. Nonessential medications included antihypertensives, antiplatelets, lipid-lowering medications, vitamins, and an antidiabetic. Medication de-escalation was not performed in 10 patients and was not warranted for the rest of the patients.
About two-thirds of the patients in the study died from a metastatic lung malignancy, followed by metastatic colorectal cancer, metastatic pancreatic cancer, and metastatic prostate cancer. None of the patients in the study died from metastatic melanoma.
Discussion
Only 1 of 57 participants was a woman. This distribution is consistent with the gender distribution in the overall population of veterans. According to the VA (2020), as of September 2019, it is estimated that there are 11,839,209 surviving male veterans aged 50 to 85 years or older as compared to 977,210 surviving female veterans from the same age groups. All of the patients in the study had access to inpatient and outpatient palliative care services. At the John D. Dingell VA Medical Center, patients diagnosed with a metastatic malignancy are automatically referred to palliative care for additional management. According to Temel et al.’s (2010) study, patients who receive early palliative care have improved quality of life, report less depression, receive less aggressive care, and have improved overall survival. As compared to the majority of the available data from the literature, there is less use of chemotherapy within 30 and 14 days of death, less aggressive care within 30 days (as defined by an emergency department visit, hospitalization, or ICU admission), and more timely hospice use in the current study (see Table 2). 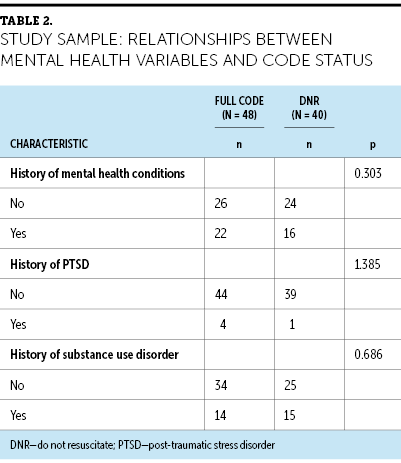
Metastatic lung malignancy was the leading cause of death among patients included in the current study, followed by metastatic colorectal cancer. This is consistent with the U.S. cancer mortality data from 2013–2017 (SEER, 2020). An ECOG score of 2 was common among the patients, which meets guidelines set forth by ASCO that recommend against the use of chemotherapy for solid tumors among patients with an ECOG score of 3 or more (Prigerson et al., 2015). Twenty-four patients in the current study received anywhere from third- to fifth-line therapy, and 19 received only one antineoplastic agent from the time of diagnosis to death. According to Prigerson et al. (2015), ECOG score is a strong determinant for receiving palliative chemotherapy in the majority of patients, which may explain why many of the patients who were included in the current study met the criteria for receiving multiple lines of therapy.
Although emergency department visits and hospitalizations within 30 days of death were still somewhat high at 44% (n = 25) and 40% (n = 23), respectively, for the patients included in the study, these numbers are lower when compared to the general population (Ersek et al., 2017). The majority of study participants went on to survive for more than a year after being diagnosed with metastatic disease while receiving oncology and palliative care services. The majority of patients were referred to hospice care prior to death and more than 30 days prior to death, with most of the referrals initiated by palliative care. These numbers are much higher when compared to trends reflected in the literature (Rhodes et al., 2019). The accessibility of inpatient and outpatient palliative care services for patients included in the current study may have influenced the greater number of patients benefiting from its services, including fewer emergency department visits and hospitalizations within 30 days of death, an increase in hospice referrals, death more than 30 days after being referred for hospice care, and less use of antineoplastic therapy within 30 and 14 days of death. The number of patients found to be taking nonessential medications in this study was also much lower than what is shown in the literature (Lindsay et al., 2015).
Limitations
This study has several limitations, including a small sample size of 57 patients that largely consisted of older adult male patients and may not be representative of the general population. The variability of the primary site for the metastatic malignancies included in this study also fails to provide a direct comparison to data available in the literature, which consisted largely of lung malignancies. It also did not account for histologic types of lung cancer. Small cell lung cancer accounts for about 15%–20% of all cases of lung cancer, and about two-thirds of patients have extensive disease with metastases at the time of diagnosis (Mouri et al., 2019). Small cell lung cancer is an aggressive malignancy but is very sensitive to the therapeutic effects of chemotherapy even though the duration of response is relatively short. Some study participants diagnosed with small cell lung cancer may have received antineoplastic therapy within 30 and 14 days of death not only to prolong life, but also to manage symptoms and improve quality of life.
The John D. Dingell VA Medical Center allows for concurrent hospice and aggressive care as long as services are not duplicated and care is coordinated between the hospice agency and the VA (Haverhals et al., 2019). Patients at the VA who are receiving hospice care can continue to see their primary care providers for comorbid conditions and can continue to receive treatment for these conditions using medications. This may have influenced the continued use of nonessential medications within 30 days of death. Additional studies evaluating these variables in relation to the findings will be helpful.
The number of emergency department visits and hospitalizations among patients in the study may not be an accurate representation of palliative care’s inability to minimize aggressive care. The inpatient hospice unit in the John D. Dingell VA Medical Center is located within the same facility as its emergency department and acute care hospital. Patients who could no longer be safely cared for at home sometimes present in the emergency department and are subsequently admitted to the hospital while awaiting admission to the inpatient hospice unit, which is subject to bed availability.
Implications for Practice
The findings from this study are consistent with the known benefits of palliative care in the comprehensive care of patients with cancer. Nurses are an integral part of that care team. At the John D. Dingell VA Medical Center, nurses assist with performing initial symptom evaluation by inquiring about the patients’ symptoms (e.g., pain, dyspnea, lightheadedness) at check-in while vital signs are being obtained. Reported symptoms are relayed to palliative care and oncology providers for further evaluation at the time of visit.
Nurses also coordinate oncology and palliative care services to ensure that patients are seen for their appointments or for any new or uncontrolled symptoms while in the chemotherapy unit for their infusions. Concerns related to lack of social support for patients are also relayed by the nurses to the social worker of the palliative care team for assistance.
A dedicated palliative care case manager who is also an RN is available for patients and their caregivers to contact for questions regarding their medications, equipment, and appointments. The case manager also provides emotional support to patients and their families. This may prevent unnecessary visits to the emergency department because of missed appointments. Missed appointments may result in running out of medications to treat symptoms, poorly controlled symptoms, and safety concerns at home.
The advanced practice nurse practitioner is also involved in the provision of palliative care services in the clinic. A dedicated nurse practitioner clinic is available to patients for outpatient palliative care consultation and follow-up, as well as transition to hospice care. Interprofessional visits that include the palliative care social worker are typically conducted with a focus on goals-of-care discussions and symptom management. The nurse practitioner also serves as a resource to other cancer care providers for information pertaining to palliative care and hospice. 
Conclusion
This study shows the use of antineoplastic therapy and aggressive care within 30 and 14 days of death at the John D. Dingell VA Medical Center were lower as compared to the available data in the literature, which could have been influenced by all of the patients having received palliative care services as part of their comprehensive cancer care in the setting of a metastatic malignancy. The use of nonessential medications near the end of life was also significantly lower compared to non-veteran patients described in the literature. Palliative care involvement may have led to improved goals-of-care discussions and enhanced symptom management that resulted in lower use of aggressive care near the end of life, as well as earlier hospice care referrals. This supports the findings in the literature that palliative care use results in improved quality of care of patients with cancer at the end of life. This can also minimize cost of care related to unnecessary procedures and medications and decrease the burden of unnecessary treatment to patients and the healthcare system.
These findings indicate the need for conducting a larger study on the benefits of palliative care involvement in minimizing the use of chemotherapy, aggressive care, and unnecessary medications within 30 days of death. Findings from this study also support the inclusion of palliative care services to improve the care of patients with cancer.
About the Author(s)
Grace Cullen, DNP, FNP-BC, AOCNP®, ACHPN®, RN-BC, is a hematology/oncology and palliative care/hospice nurse practitioner at John D. Dingell VA Medical Center in Detroit, MI. The author takes full responsibility for this content and did not receive honoraria or disclose any relevant financial relationships. The article has been reviewed by independent peer reviewers to ensure that it is objective and free from bias. Cullen can be reached at grace.cullen@va.gov, with copy to CJONEditor@ons.org. (Submitted February 2020. Accepted June 22, 2020.)
References
Bao, Y., Maciejewski, R.C., Garrido, M.M., Shah, M.A., Maciejewski, P.K., & Prigerson, H.G. (2018). Chemotherapy use, end-of-life care, and costs of care among patients diagnosed with Stage IV pancreatic cancer. Journal of Pain and Symptom Management, 55(4), 1113–1121. https://doi.org/10.1016/j.painsymman.2017.12.335
Clarke, G., Johnston, S., Corrie, P., Kuhn, I., & Barclay, S. (2015). Withdrawal of anticancer therapy in advanced disease: A systematic literature review. BMC Cancer, 15, 892. https://doi.org/10.1186/s12885-015-1862-0
Ersek, M., Miller, S.C., Wagner, T.H., Thorpe, J.M., Smith, D., Levy, C.R., . . . Mor, V. (2017). Association between aggressive care and bereaved families’ evaluation of end-of-life care for veterans with non-small cell lung cancer who died in Veterans Affairs facilities. Cancer, 123(16), 3185–3194. https://doi.org/10.1002/cncr.30700
Green, J.B., Shapiro, M.F., Ettner, S.L., Malin, J., Ang, A., & Wong, M.D. (2017). Physician variation in lung cancer treatment at the end of life. American Journal of Managed Care, 23(4), 216–223.
Haverhals, L.M., Manheim, C.E., Mor, V., Ersek, M., Kinosian, B., Lorenz, K.A., . . . Levy, C. (2019). The experience of providing hospice care concurrent with cancer treatment in the VA. Supportive Care in Cancer, 27(4),1263–1270. https://doi.org/10.1007/s00520-018-4552-z
Lindsay, J., Dooley, M., Martin, J., Fay, M., Kearney, A., Khatun, M., & Barras, M. (2015). The development and evaluation of an oncological palliative care deprescribing guideline: The “OncPal deprescribing guideline.” Supportive Care in Cancer, 23(1), 71–78. https://doi.org/10.1007/s00520-014-2322-0
Mack, J.W., Chen, K., Boscoe, F.P., Gesten, F.C., Roohan, P.J., Schymura, M.J., & Shrag, D. (2015). High intensity of end-of-life care among adolescent and young adult cancer patients in the New York State Medicaid program. Medical Care, 53(12), 1018–1026. https://doi.org/10/1097/MLR.0000000000000437
Margolis, B., Chen, L., Accordino, M.K., Clarke Hillyer, G., Hou, J.Y., Tergas, A.I., . . . Wright, J.D. (2017). Trends in end-of-life care and healthcare spending in women with uterine cancer. American Journal of Obstetrics and Gynecology, 217(4), 434.e1–434.e10. https://doi.org/10.1016/j.ajog.2017.07.006
Mor, V., Joyce, N.R., Coté, D.L., Gidwani, R.A., Ersek, M., Levy, C.R., . . . Shreve, S.T. (2016). The rise of concurrent care for veterans with advanced cancer at the end of life. Cancer, 122(5), 781–795. https://doi.org/10.1002/cncr.29827
Mouri, A., Yamaguchi, O., Miyauchi, S., Shiono, A., Utsugi, H., Nishihara, F., . . . Kobayashi, K. (2019). Combination therapy with carboplatin and paclitaxel for small cell lung cancer. Respiratory Investigation, 57(1),34–39. https://doi.org/10.1016/j.resinv.2018.09.004
Oken, M.M., Creech, R.H., Tormey, D.C., Horton, J., Davis, T.E., McFadden, E.T., & Carborne, P.P. (1982). Toxicity and response criteria of the Eastern Cooperative Oncology Group. American Journal of Clinical Oncology, 5(6), 649–655.
Prigerson, H.G., Bao, Y., Shah, M.A., Paulk, M.E., LeBlanc, T.W., Schneider, B.J., . . . Maciejewski, P.K. (2015). Chemotherapy use, performance status, and quality of life at the end of life. JAMA Oncology, 1(6), 778–784. https://doi.org/10.1001/jamaoncol.2015.2378
Rhodes, R.L., Ukoha, N.C.E., Williams, K.A., Elwood, B., Knox-Rice, T., Lee, S.C., . . . Halm, E.A. (2019). Understanding underuse of advance care planning among a cohort of African American patients with advanced cancer: Formative research that examines gaps in intent to discuss options for care. American Journal of Hospice and Palliative Medicine, 36(12), 1057–1062. https://doi.org/10.1177/1049909119843276
Surveillance, Epidemiology, and End Results Program. (2020). Table 1.1: Estimated new cancer cases and deaths for 2020—All races, by sex [Dataset]. National Cancer Institute. https://seer.cancer.gov/csr/1975_2017/results_single/sect_01_table.01.p…
Temel, J.S., Greer, J.A., Muzikansky, A., Gallagher, E.R., Admane, S., Jackson, V.A., . . . Lynch, T.J. (2010). Early palliative care for patients with metastatic non-small-cell lung cancer. New England Journal of Medicine, 363(8), 733–742. https://doi.org/10.1056/NEJMoa1000678
U.S. Department of Veterans Affairs. (2020). National Center for Veterans Analysis and Statistics. https://www.va.gov/vetdata/Veteran_Population.asp


